
48 results
24-Hour warning signs for adolescent suicide attempts
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 7 / May 2024
- Published online by Cambridge University Press:
- 10 November 2023, pp. 1272-1283
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Large eddy simulations of bubbly flows and breaking waves with smoothed particle hydrodynamics
-
- Journal:
- Journal of Fluid Mechanics / Volume 972 / 10 October 2023
- Published online by Cambridge University Press:
- 03 October 2023, A24
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Clinical factors and diagnoses associated with inappropriate urine-culture ordering in primary care
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Integrating the “Quit and Stay Quit Monday” Model into Smoking Cessation Services for Smokers with Mental Health Conditions: A Pilot Randomized Controlled Trial
-
- Journal:
- Journal of Smoking Cessation / Volume 2023 / 2023
- Published online by Cambridge University Press:
- 01 January 2024, e2
- Print publication:
- 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 24 - Fundamentals of Decontamination and Sterilisation
-
-
- Book:
- Fundamentals of Operating Department Practice
- Published online:
- 18 August 2022
- Print publication:
- 08 September 2022, pp 264-273
-
- Chapter
- Export citation
Prior cultures predict subsequent susceptibility in patients with recurrent urinary tract infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s67
-
- Article
-
- You have access
- Open access
- Export citation
-
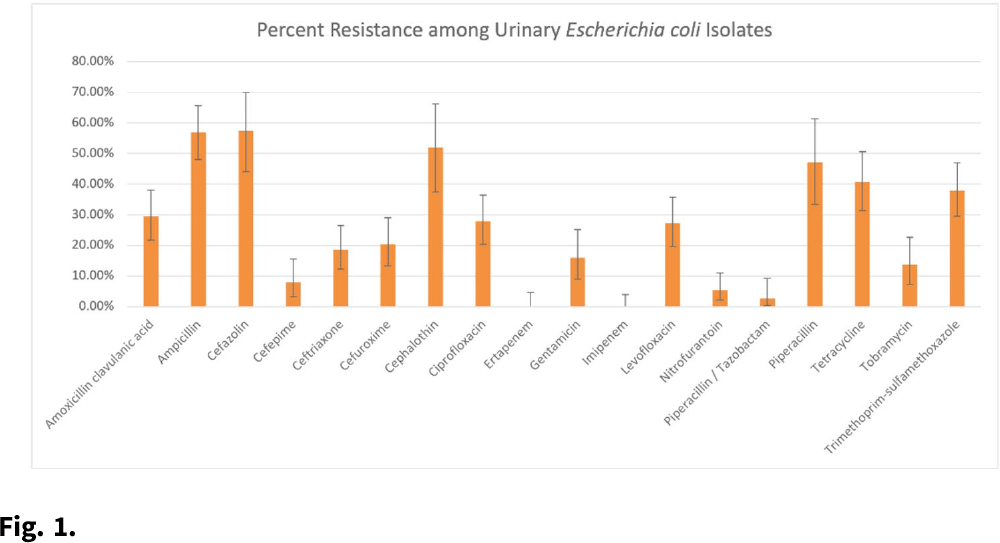
Background: Patients with recurrent urinary tract infections (rUTI) experience frequent exposure to antimicrobial regimens, leaving them at higher risk for developing antibiotic resistance. Little information on the prevalence of antibiotic resistance among patients with rUTI has been published. Although the IDSA recommends using a prior culture to guide empiric treatment, studies have not examined the predictive ability of a prior culture among patients meeting rUTI criteria. We constructed an antibiogram and evaluated test metrics, including sensitivity, specificity, and positive predictive value (PPV) and negative predictive values (NPV) of a prior culture (any organism), on predicting resistance (PPV) or susceptibility (NPV) of a future culture among patients with uncomplicated rUTI in an outpatient setting. Methods: We retrospectively extracted electronic health record data from outpatients aged ≥18 years who had an ICD-10 code for cystitis listed twice in 6 months or thrice in 12 months between November 1, 2016, and December 31, 2018. Patients sought care at either urology or primary care practices within an academic medical center in Houston, Texas. Patients with functional or structural abnormalities of the genitourinary tract, signs or symptoms of pyelonephritis, or pregnancy were excluded. Antibiogram data were reported for uropathogens with ≥30 isolates, and intermediate results were considered resistant. Test metrics and Bayes’ PPV and NPV were calculated using standard formulas. Results: We included 597 visits from 232 unique patients. Most were White (63%) and female (92%), and the cohort had a median age of 58 (IQR, 41–68). Among 310 rUTI episodes with a urine culture, 189 (61%) had at least 1 uropathogen isolated, and Escherichia coli (n = 130, 66%) was most common among all 196 uropathogens. E. coli isolates had >20% resistance to 10 of 18 antibiotics (Fig. 1). E. coli resistance to ciprofloxacin was 27.9%, resistance to nitrofurantoin was 5.5%, and resistance to trimethoprim-sulfamethoxazole was 38.0%. The PPVs for predicting resistance were highest for ceftriaxone (0.86; 95% CI, 0.60–0.96), ciprofloxacin (0.84; 95% CI, 0.63–0.94), and levofloxacin (0.84; 95% CI, 0.63–0.94). NPVs of resistance were highest for gentamicin (0.97; 95% CI, 0.83–1.00), ceftriaxone (0.94; 95% CI, 0.86–0.98), and cefepime (0.94; 95% CI, 0.84–0.98), whereas NPVs for cefuroxime, ciprofloxacin, levofloxacin, and nitrofurantoin were all >0.83. Conclusions: We detected considerable antibiotic resistance among patients with rUTI to commonly prescribed antibiotics. Prior urine culture susceptibility demonstrated moderate-to-high PPVs for predicting future resistance to ceftriaxone and fluoroquinolones as well as high NPVs for several cephalosporins and fluoroquinolones, which could inform empiric prescribing choices.
Funding: This investigator-initiated research study was funded by Rebiotix, a Ferring Company.
Disclosures: None

Effectiveness and optimal duration of early intervention treatment in adult-onset psychosis: a randomized clinical trial
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 6 / April 2023
- Published online by Cambridge University Press:
- 11 February 2022, pp. 2339-2351
-
- Article
- Export citation
Analysis of recurrent urinary tract infection management in women seen in outpatient settings reveals opportunities for antibiotic stewardship interventions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 17 January 2022, e8
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Analysis of Recurrent Urinary Tract Infection Management in Outpatient Settings Reveals Opportunities for Antibiotic Stewards
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s34
-
- Article
-
- You have access
- Open access
- Export citation
A comparison of self-reported risk and protective factors and the death implicit association test in the prediction of future suicide attempts in adolescent emergency department patients
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 1 / January 2023
- Published online by Cambridge University Press:
- 05 May 2021, pp. 123-131
-
- Article
- Export citation
Racial Reparations against White Protectionism: America's New Racial Politics
-
- Journal:
- Journal of Race, Ethnicity and Politics / Volume 6 / Issue 1 / March 2021
- Published online by Cambridge University Press:
- 05 January 2021, pp. 82-96
-
- Article
- Export citation
APSA Presidential Task Force Report on New Partnerships
-
- Journal:
- PS: Political Science & Politics / Volume 53 / Issue 4 / October 2020
- Published online by Cambridge University Press:
- 16 October 2020, pp. 847-849
- Print publication:
- October 2020
-
- Article
-
- You have access
- HTML
- Export citation
The 12-month prevalence of psychotic experiences and their association with clinical outcomes in Hong Kong: an epidemiological and a 2-year follow up studies
-
- Journal:
- Psychological Medicine / Volume 51 / Issue 14 / October 2021
- Published online by Cambridge University Press:
- 29 May 2020, pp. 2501-2508
-
- Article
- Export citation
White Protectionism in America
-
- Journal:
- Perspectives on Politics / Volume 19 / Issue 2 / June 2021
- Published online by Cambridge University Press:
- 13 May 2020, pp. 460-478
- Print publication:
- June 2021
-
- Article
-
- You have access
- HTML
- Export citation
Differentiation of turfgrass and common weed species using hyperspectral radiometry
-
- Journal:
- Weed Science / Volume 54 / Issue 2 / April 2006
- Published online by Cambridge University Press:
- 20 January 2017, pp. 335-339
-
- Article
- Export citation
THE LAST STAND?: Shelby County v. Holder, White Political Power, and America’s Racial Policy Alliances
-
- Journal:
- Du Bois Review: Social Science Research on Race / Volume 13 / Issue 1 / Spring 2016
- Published online by Cambridge University Press:
- 13 May 2016, pp. 25-44
-
- Article
- Export citation
Suicide by people in a community justice pathway: Population-based nested case–control study
-
- Journal:
- The British Journal of Psychiatry / Volume 207 / Issue 2 / August 2015
- Published online by Cambridge University Press:
- 02 January 2018, pp. 175-176
- Print publication:
- August 2015
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Clinical Gynecology
- Published online:
- 05 April 2015
- Print publication:
- 23 April 2015, pp viii-xiv
-
- Chapter
- Export citation
Use of vitamin D supplements during infancy in an international feeding trial
-
- Journal:
- Public Health Nutrition / Volume 17 / Issue 4 / April 2014
- Published online by Cambridge University Press:
- 24 June 2013, pp. 810-822
-
- Article
-
- You have access
- HTML
- Export citation
